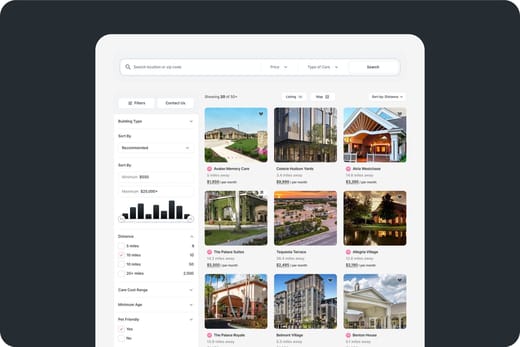
Deficiencies (last 4 years)
Deficiencies (over 4 years)
9 deficiencies/year
Deficiencies are regulatory violations found during state inspections.
73% worse than New Jersey average
New Jersey average: 5.2 deficiencies/yearDeficiencies per year
28
21
14
7
0
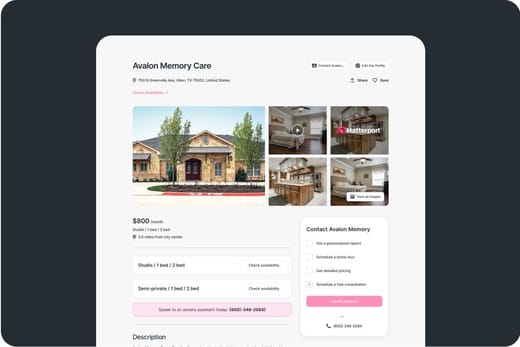
Occupancy
Latest occupancy rate
11% occupied
Based on a November 2025 inspection.
This facility has shown a decline in demand based on occupancy rates.
Occupancy rate over time
Inspection Report
Complaint Investigation
Census: 17
Deficiencies: 1
Date: Nov 21, 2025
Visit Reason
The inspection was conducted due to a complaint investigation regarding the facility's failure to provide appropriate quality of care related to intravenous antibiotic medication administration for one resident.
Complaint Details
Complaint #437202 involved failure to ensure Resident 3 received timely IV antibiotic medication, with missed doses from 05/21/25 through 05/24/25. The facility did not notify the physician promptly, and the resident's records did not reflect physician awareness until 05/29/25. The nursing home disputes the citation.
Findings
The facility failed to administer IV Cefazolin antibiotic medication to Resident 3 as ordered for four consecutive days, resulting in delayed treatment for osteomyelitis. The resident's physician was not timely informed of the missed doses, and documentation did not reflect awareness or plans to address the missed medication administration.
Deficiencies (1)
Failure to provide appropriate quality of care related to intravenous antibiotic medication administration resulting in missed doses for Resident 3.
Report Facts
Residents reviewed in sample: 17
Missed antibiotic doses: 4
Resident age: 73
Employees mentioned
| Name | Title | Context |
|---|---|---|
| Vice President of Clinical Services (VPCS) | Interviewed and confirmed expectations regarding physician awareness of missed antibiotic doses | |
| Director of Nursing (DON) | Interviewed and confirmed awareness of delayed IV antibiotic administration and physician notification expectations |
Notice
Deficiencies: 0
Date: Nov 19, 2025
Visit Reason
This document serves to inform individuals about the privacy practices of NJDHSS, including how their medical information may be used and disclosed, and their rights related to this information.
Findings
The notice details the types of information covered, reasons for use and disclosure of health information, individuals' rights to access and control their information, and the legal duties of NJDHSS to protect privacy.
Report Facts
Effective date: 2011
Employees mentioned
| Name | Title | Context |
|---|---|---|
| Devon L. Graf | Director, Office of Legal and Regulatory Compliance | Listed as NJDHSS Privacy Officer contact for questions about the notice |
Inspection Report
Routine
Census: 89
Deficiencies: 0
Date: Nov 27, 2024
Visit Reason
A COVID-19 Focused Infection Control Survey was conducted by the State Agency to assess compliance with New Jersey Administrative Code 8:36 infection control regulations and CDC recommended practices.
Findings
The facility was found to be in compliance with the infection control regulations and CDC recommended practices to prepare for COVID-19.
Report Facts
Sample Size: 3
Inspection Report
Complaint Investigation
Census: 126
Deficiencies: 6
Date: Sep 20, 2024
Visit Reason
The inspection was conducted based on complaints regarding failure to notify resident representatives and physicians timely of changes in condition, inaccurate Minimum Data Set (MDS) coding, failure to obtain physician orders for discharge, lack of discharge summary, inadequate pain management, and insufficient nursing staff with delayed call bell responses.
Complaint Details
Complaints NJ#175244, NJ174669, NJ175260, and NJ176352 involved failure to notify representatives and physicians timely, inaccurate MDS coding, discharge planning deficiencies, inadequate pain management, and insufficient staffing with delayed call bell responses.
Findings
The facility failed to notify the resident's representative and physician timely after an incident, inaccurately coded MDS assessments for multiple residents, failed to obtain physician orders for discharge and document acceptance of home care referrals, lacked a discharge summary for a discharged resident, did not consistently assess and document pain for a cognitively impaired resident, and had insufficient nursing staff leading to delayed call bell responses.
Deficiencies (6)
Failure to notify resident's representative and physician of change in condition in a timely manner for Resident #209.
Failure to accurately code the Minimum Data Set (MDS) for Residents #62, #148, and #209.
Failure to obtain physician's order for discharge and document acceptance of home care referral for Resident #308.
Failure to provide a discharge summary for Resident #308.
Failure to ensure consistent pain assessment and management for Resident #209.
Insufficient nursing staff and delayed call bell responses for multiple residents including Residents #36, 60, 83, 84, 100, 102, and 153.
Report Facts
Resident census: 126
CNA to resident ratio: 9
Call bell response times: 20
Pain assessment frequency: 3
Pain assessment frequency: 6
Pain assessment frequency: 2
Call bell audit wait times: 25
Employees mentioned
| Name | Title | Context |
|---|---|---|
| RN/MDS Coordinator #1 | Registered Nurse/MDS Coordinator | Interviewed regarding MDS coding discrepancies |
| Licensed Practical Nurse (LPN) | Unit Manager/Licensed Practical Nurse | Interviewed regarding pain assessment practices |
| Social Worker Director (SWD) | Social Worker Director | Interviewed regarding discharge planning and home care referral process |
| Director of Nursing | Director of Nursing (DON) | Interviewed regarding pain management and notification practices |
| Licensed Nursing Home Administrator | LNHA | Interviewed regarding call bell system and discharge planning |
| Business Development Coordinator | Business Development Coordinator for Home Care Service Agency #1 | Interviewed regarding home care referral acceptance and communication |
Inspection Report
Complaint Investigation
Census: 120
Deficiencies: 19
Date: Sep 20, 2024
Visit Reason
The inspection was complaint-related, triggered by allegations regarding failure to notify resident representatives and physicians timely, inaccurate assessments, medication errors, and other care concerns.
Complaint Details
Complaint NJ#175244 and others related to notification failures, MDS inaccuracies, medication errors, infection control, staffing, and resident care.
Findings
The facility was found deficient in timely notification of resident condition changes, inaccurate MDS coding, failure to monitor and document post-fall conditions, medication administration errors, incomplete assessments, infection control lapses, inadequate staffing, missing discharge documentation, and failure to offer pneumococcal vaccines.
Deficiencies (19)
Failure to notify resident's representative and physician of change in condition in a timely manner for Resident #209.
Failure to accurately code the Minimum Data Set (MDS) for three residents including Resident #209.
Failure to monitor and document neurochecks and post-fall condition for Resident #148.
Failure to follow physician's order and document urinary catheter output for Resident #358.
Medication administration error: administering tablet form instead of ordered capsule for Resident #260.
Failure to obtain physician's order for discharge and document approval for home care referral for Resident #308.
Failure to provide appropriate pressure ulcer care and documentation for Resident #36.
Failure to provide appropriate care to maintain or improve range of motion for Resident #67.
Failure to administer oxygen therapy according to physician's order and improper storage of respiratory equipment for multiple residents.
Failure to provide safe and appropriate pain management for Resident #209, including lack of routine pain assessments.
Failure to maintain dialysis communication records and provide adequate dialysis care for Residents #458 and #98.
Failure to post nurse staffing information daily and ensure sufficient nursing staff to meet resident needs.
Failure to ensure medications are stored securely and not left unattended on medication carts.
Failure to maintain kitchen sanitation and safe food handling practices, including unlabeled food and improper sanitizing.
Failure to maintain accurate and complete medical records, including conflicting documentation of code status for Resident #62.
Failure to follow infection prevention and control practices including hand hygiene, PPE use, and wound care procedures.
Failure to offer pneumococcal vaccine or document reason for ineligibility for Residents #43, #62, and #148.
Failure to maintain complete, accurate, and accessible medical records for Residents #62 and #148.
Failure to provide designated dining room and dining activities for residents as approved in facility plan.
Report Facts
Resident census: 120
Nurse aide to resident ratio: 8.6
Nurse aide to resident ratio: 9
Weight: 165
Weight: 184.8
Weight: 190.8
Weight: 160.2
Weight: 125.6
Weight: 125
Weight: 125
Weight: 125
Weight: 124
Weight: 126.1
Weight: 126.8
Weight: 128.6
Staffing: 16
Employees mentioned
| Name | Title | Context |
|---|---|---|
| Licensed Practical Nurse #1 | LPN | Mentioned in relation to notification failure and infection control lapses |
| Licensed Nursing Home Administrator | LNHA | Facility management and interviewee for multiple findings |
| Director of Nursing | DON | Facility management and interviewee for multiple findings |
| Assistant Director of Nursing/Infection Preventionist | ADON/IP | Facility management and interviewee for infection control and other findings |
| Regional Nurse Consultant #1 | RNC#1 | Facility management and interviewee for multiple findings |
| Registered Nurse #1 | RN | Observed medication administration error |
| Certified Nursing Aide #1 | CNA | Observed infection control lapses |
| Certified Nursing Aide #2 | CNA | Observed infection control lapses |
| Consultant Pharmacist | CP | Interviewed regarding medication administration and infection control |
| Physiatrist | Physician | Interviewed regarding range of motion care |
| Director of Rehabilitation | DoR/OT | Interviewed regarding therapy screening and care |
| Social Worker Director | SWD | Interviewed regarding discharge planning |
| Registered Nurse/MDS Coordinator #1 | RN/MDSC | Interviewed regarding MDS coding and assessments |
Inspection Report
Deficiencies: 1
Date: Feb 12, 2024
Visit Reason
The inspection was conducted to evaluate the facility's compliance with care plan requirements, specifically regarding the completion and updating of care plans for residents at risk for falls.
Findings
The facility failed to complete and update the care plan for a resident at risk for falls, despite a fall incident occurring during the review period. The care plan did not reflect interventions related to the fall, and the Assistant Director of Nursing was unable to explain this omission.
Deficiencies (1)
Failed to complete and update the care plan for a resident at risk for falls, not reflecting interventions related to a fall incident.
Inspection Report
Routine
Deficiencies: 6
Date: Aug 15, 2023
Visit Reason
The inspection was conducted to assess compliance with federal and state regulations regarding resident assessments, medication administration, nutrition monitoring, feeding tube care, and pharmacy consultant recommendations at Livingston Post Acute Care.
Findings
The facility was found deficient in multiple areas including late transmission of Minimum Data Set (MDS) assessments, inaccurate MDS coding, improper administration of medication contrary to physician orders, failure to obtain weekly weights as ordered, inadequate monitoring of enteral feeding volumes, and failure to act on pharmacy consultant recommendations within an acceptable timeframe.
Deficiencies (6)
Failed to complete and transmit Minimum Data Set (MDS) Entry Reporting Assessments within required timeframes for 2 of 38 residents.
Failed to accurately code MDS assessments for 3 of 22 residents, including incorrect discharge status and inaccurate weight loss coding.
Failed to properly administer Midodrine medication according to physician's order for 1 of 22 residents, administering medication when blood pressure exceeded ordered parameters.
Failed to obtain weekly weights as ordered for 1 of 5 residents, missing weights for four weeks.
Failed to monitor enteral feeding pump to assure total volume administered matched physician's order for 1 of 3 residents, resulting in incomplete feeding volumes.
Failed to act upon pharmacy consultant recommendations within an acceptable timeframe for 1 of 38 residents, with recommendations not reviewed or addressed.
Report Facts
Residents reviewed for MDS transmission: 38
Residents reviewed for MDS coding accuracy: 22
Residents reviewed for medication administration: 22
Residents reviewed for nutrition monitoring: 5
Residents reviewed for enteral feeding: 3
Residents reviewed for pharmacy consultant follow-up: 38
Total volume ordered for enteral feeding: 1560
Weight loss: 5
Employees mentioned
| Name | Title | Context |
|---|---|---|
| Registered Nurse (RN) MDS Coordinator | Responsible for completing and transmitting MDS assessments; acknowledged late transmissions | |
| RN President of Clinical Services | Discussed concerns regarding MDS assessments and enteral feeding discrepancies | |
| MDS Coordinator #1 | Explained incorrect MDS coding due to wrong button selection | |
| MDS Coordinator #2 | Acknowledged inaccurate weight documentation and MDS coding errors | |
| Licensed Practical Nurse (LPN) | Acknowledged expectation to follow medication orders and BP parameters | |
| Licensed Practical Nurse/Unit Manager (LPN/UM) | Acknowledged medication administration errors and responsibility for weight documentation | |
| Certified Nursing Assistant (CNA) | Provided information on weight obtaining process | |
| Registered Dietician (RD) | Responsible for reviewing resident weights and providing weight lists | |
| Regional Registered Dietician (RRD) | Participated in interview regarding weight monitoring | |
| Registered Nurse (RN) assigned to Resident #391 | Provided information on enteral feeding administration | |
| RN/Unit Manager (UM) | Verified feeding orders and acknowledged lack of awareness of total volume ordered | |
| Director of Nursing (DON) | Acknowledged concerns regarding weights and enteral feeding discrepancies | |
| Assistant Director of Nursing (ADON) | Acknowledged concerns regarding weights and enteral feeding discrepancies | |
| Registered Nurse/Unit Manager (RN/UM) | Confirmed pharmacy consultant recommendations were not reviewed or addressed | |
| Registered Nurse/Vice President of Clinical Services (RN/VP CS) | Confirmed pharmacy consultant recommendations were not handled |
Inspection Report
Original Licensing
Deficiencies: 1
Date: Apr 21, 2023
Visit Reason
The inspection was an initial licensing survey to determine compliance with New Jersey Administrative Code 8:36 standards for licensure of assisted living residences, comprehensive personal care homes, and assisted living programs.
Findings
The facility was found not in substantial compliance due to failure to provide an emergency generator annunciator panel in a location observable by operating staff 24 hours a day, as required by the New Jersey Uniform Construction Code for health care occupancy.
Deficiencies (1)
Failure to provide the annunciator panel for the emergency generator in a location observable by operating staff 24 hours a day, in accordance with New Jersey Uniform Construction Code, N.J.A.C. 5:23, for use group I-2 (health care) occupancy.
Report Facts
Census: 0
Employees mentioned
| Name | Title | Context |
|---|---|---|
| Corporate Director of Environmental Services | Corporate Director of Environmental Services | Interviewed regarding the location and existence of the emergency generator annunciator panel |
| Executive Director | Executive Director | Interviewed during entrance conference about emergency generator |
Inspection Report
Routine
Deficiencies: 2
Date: Jun 21, 2021
Visit Reason
The inspection was conducted to evaluate the facility's compliance with regulations related to fall prevention and medication labeling and storage.
Findings
The facility failed to consistently implement interventions to prevent falls for a resident requiring 1:1 care, and failed to properly label and date medications in three of six medication carts inspected, posing minimal harm or potential for actual harm.
Deficiencies (2)
Failed to consistently implement interventions to prevent falls for Resident #30 who required 1:1 care and was found unattended and unsupervised.
Failed to properly label and date medications in three of six medication carts, including unlabeled insulin pens and medications beyond discard dates.
Report Facts
Medication carts inspected: 6
Medication carts with labeling deficiencies: 3
Residents reviewed for falls: 1
Falls without injury since admission: 1
Employees mentioned
| Name | Title | Context |
|---|---|---|
| CNA #2 | Certified Nursing Assistant | Named in fall prevention deficiency for being inattentive and possibly fatigued during 1:1 care |
| LPN #3 | Licensed Practical Nurse | Named in medication labeling deficiency for not noticing unlabeled medication bottles |
| LPN #1 | Licensed Practical Nurse | Named in medication labeling deficiency related to inspection of medication cart |
| LPN #2 | Licensed Practical Nurse | Named in medication labeling deficiency for not noticing unlabeled insulin pen and bag |
| Registered Nurse Unit Manager | Registered Nurse Unit Manager | Involved in supervising and responding to fall prevention incident |
| Director of Nursing | Director of Nursing | Provided facility policy and procedure for falls and fall risk management |
| Regional Registered Nurse | Regional Registered Nurse | Provided facility investigation and packing slip related to medication labeling issues |
Viewing
Loading inspection reports...
